Endoscopy is an important technique for medical diagnosis. Endoscopes, small cameras, are inserted into patients via natural holes or small artificial incisions to examine hollow organs or cavities within the body. To perform surgery or take tissue probes, a second device, such as tiny scissors or forceps, can be inserted along with the endoscope. Since endoscopic procedures are associated with discomfort for the patients, it is important to keep them as short as possible by working efficiently. Virtual endoscopy is a relatively new method of diagnosis, which provides simulated visualizations of inner organs similar or equivalent to those produced by standard endoscopic procedures and can support the endoscopist in many ways. It is performed by placing a virtual camera into a three dimensional data volume which most commonly is acquired from computer tomography (CT) or magnetic resonance imaging (MRI). Data acquisition is therefore non-invasive and causes almost no discomfort for the patient. Another advantage of virtual over physical endoscopy is the extended field of view: the virtual endoscope can easily be adjusted to point in any direction. Furthermore, the field of view needs not be confined by organ walls, instead, also external structures can be viewed. If no physical interference is required at all, virtual endoscopy might even in some cases replace the real endoscopic procedure. Otherwise, it is still a powerful tool which can aid the endoscopist to identify regions of interest within the investigated organ prior to a real endoscopic examination or to navigate the physical endoscope through a widely branched organ.
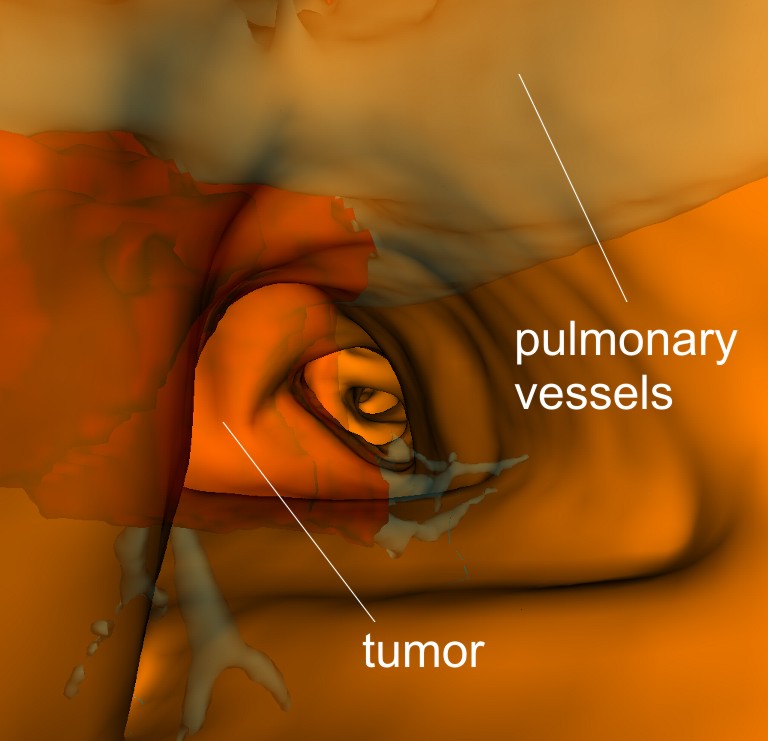
An interesting application of endoscopy is trans-bronchial biopsy. If a tumor is detected inside a patient's lung, a device has to be inserted into the body to take a biopsy from tumor tissue, which is then tested for malignity. Tumors are often hidden behind bronchial walls and therefore cannot be seen through a camera inserted into the bronchial tree. Also, bronchial walls occlude the aorta and other important blood vessels that must not take any damage during the biopsy. A virtual camera, however, can display the bronchial walls semi-transparently and thus guide the physicist to the tumor and help them find the correct position for biopsy. In this application, virtual endoscopy can be carried out either prior to the real endoscopic procedure as an exercise for the endoscopist, or even during the physical examination as a navigation aid. There is no doubt that especially in the latter case, virtual endoscopy must not induce any artificial delays. The process of rendering the virtual camera image should be fast. An elaborate visualization technique, which displays the surface of the organ under investigation semi-transparently and specified objects of interest (here: the tumor and the vessel tree) opaquely (see figure 1) within reasonable frame times, is needed.
Cell-based first-hit ray casting, a new volume visualization technique suitable for a large variety of virtual endoscopy scenarios, is presented and evaluated with respect to the trans-bronchial biopsy application in this paper.